


Overview
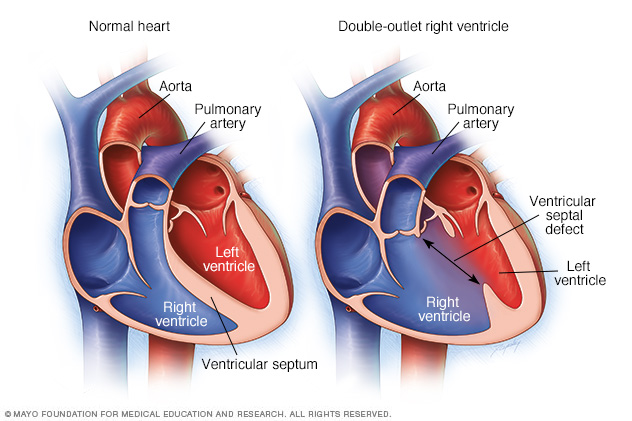
Double-outlet right ventricle is a heart condition present at birth. That means it's a congenital heart defect. In this condition, the lower right heart chamber has two openings for blood to exit the heart instead of one. Some of the blood from the lower right heart chamber goes to the body instead of the lungs.
Babies with double-outlet right ventricle also have a hole between the lower heart chambers. The lower heart chambers are called the ventricles. The hole is called a ventricular septal defect. The hole causes oxygen-rich blood to mix with oxygen-poor blood. Babies with this hole may not get enough oxygen in the bloodstream. Their skin may appear gray or blue.
Double-outlet right ventricle may occur with other heart conditions present at birth such as other holes in the heart and blood vessel or heart valve changes.
Symptoms
Symptoms of double-outlet right ventricle may include:
- Pale gray or blue lips, tongue, or fingernails. Depending on skin color, these changes may be harder or easier to see.
- Rapid breathing.
- Problems with feeding, growth and weight gain.
When to see a doctor
If you think that your baby has symptoms of a heart condition, make an appointment for a health checkup right away.
Causes
The exact cause of a double-outlet right ventricle is not known. The condition happens when the unborn baby, also called a fetus, is developing before birth.
Gene changes, some medicines or health conditions, and environmental or lifestyle factors may play a role. Smoking while pregnant also may increase the risk of certain congenital heart defects in an unborn baby.
Usually, the body's main artery, called the aorta, connects to the left lower heart chamber. The pulmonary artery connects to the right lower heart chamber. But in babies with double-outlet right ventricle, both the aorta and the pulmonary artery connect partially or completely to the right lower heart chamber.
Risk factors
Having a family history of congenital heart conditions may increase the risk of congenital heart defects such as double-outlet right ventricle.
Complications
Complications of double-outlet right ventricle include poor growth and heart failure.
Diagnosis
A test called an echocardiogram can diagnose double-outlet right ventricle. The test uses sound waves to create images of the beating heart. It can show blood flow through the heart and heart valves.
If more details about the heart are needed, other tests may be done. Tests to check the heart may include:
- Heart CT scan. This also is called a cardiac CT. This test uses X-rays to create cross-sectional images of specific parts of the body.
- Heart MRI scan. This test uses magnetic fields and radio waves to create detailed pictures of the heart.
- Cardiac catheterization. A doctor places a long, thin flexible tube called a catheter into a blood vessel, usually in the groin or wrist. It's guided to the heart. Dye flows through the catheter to the heart arteries. The dye helps the arteries show up more clearly on images taken during the test. During this test, the healthcare professional also can measure pressure and oxygen levels in the chambers of the heart and in the blood vessels.
Treatment
Most babies with double-outlet right ventricle have heart repair surgery within a few months of age. More than one type of surgery may be done. The type of surgery depends on the specific heart structure.
The heart surgeon may do one or more of the following to treat double-outlet right ventricle:
- Create a pathway in the heart to connect the lower left heart chamber to the body's main artery, called the aorta.
- Use a patch, called a baffle, to fix the hole in the heart.
- Fix the aorta and pulmonary artery positions if they're reversed.
- Connect the lower right heart chamber to the pulmonary artery, if necessary.
- Widen the natural pathway to the lungs if it's narrowed.
Other surgeries might be needed later in life. A person born with double-outlet right ventricle needs regular health checkups for life. Adults should see a doctor trained in evaluating and treating congenital heart conditions. This type of doctor is called an adult congenital cardiologist.
© 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use